Authors: Jacob Flapan1, Ria Smith1, Keith Siau1
Affiliations: Gastroenterology and Liver Unit, Royal Hospital Cornwall Hospital Trust, Truro, Cornwall
Abstract
This British Society for Gastroenterology (BSG) web education article provides a pragmatic overview on the pharmacological management of acute upper gastrointestinal bleeding (AUGIB). It is aimed at frontline clinicians who manage AUGIB with focus on pre-endoscopic and post-endoscopic pharmacological interventions. Management of variceal and non-variceal AUGIB are discussed, with reference to latest evidence-based interventions and clinical guidelines.
Introduction
Acute upper gastrointestinal bleeding (AUGIB) is defined as acute bleeding from the oesophagus, stomach or duodenum proximal to the ligament of Treitz. It is a common medical emergency with an estimated mortality rate of up to 7%.[1] The facets of AUGIB management can be divided into pre-endoscopic, endoscopic and post-endoscopic care. Pre-endoscopic clinical management has been summarised in the recent BSG endoscopy acute upper GI bleed care bundle,[2] starting with early recognition, assessment and effective resuscitation.[3] Risk stratification using evidence-based scoring systems can assist with triaging potential severity of AUGIB to guide the need for admission, estimate prognosis,[4,5] and gauge timing of endoscopy which is the mainstay of treatment in AUGIB.[6] Endoscopy enables the diagnosis of underlying pathology and allows interventions under direct visualisation to achieve haemostasis in AUGIB. The endoscopic diagnosis can be used to guide pharmacological management.
Within this article, evidence-based pharmacological interventions that directly influence outcomes in AUGIB will be discussed. Although important in the management of AUGIB, supportive treatments such as blood products and fluid regimes used in resuscitation, reversal agents for anticoagulants and resumption of antithrombotics will not be covered in detail in this paper. However, the BSG has published guidance for the management of patients on anticoagulation and antiplatelet therapy, which have been included in this article (Figures 1,2).
Pragmatically, the pharmacological approach to AUGIB can be divided based upon the cause: acute variceal (AVUGIB) or non-variceal (NVUGIB). The cause can be confirmed at endoscopy, but clues in the history and examination (Figure 3) can guide pre-endoscopic management.
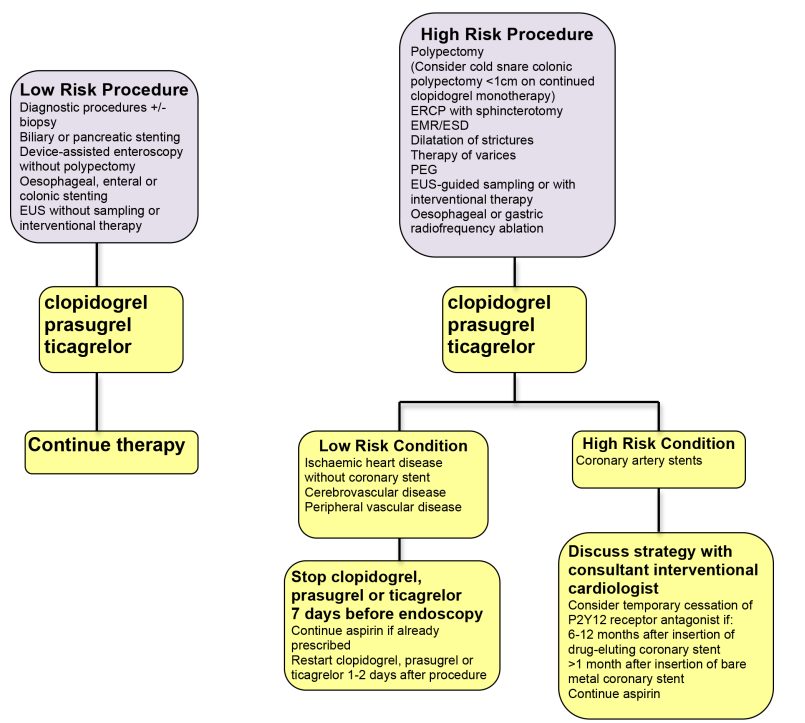
Figure 1: Guidelines for the management of patients on P2Y12 receptor antagonist antiplatelet agents undergoing endoscopic procedures: 2021 update [7]
EUS = endoscopic ultrasound, ERCP = endoscopic retrograde cholangiopancreatography, EMR = endoscopic mucosal resection, ESD = endoscopic submucosal dissection, PEG = percutaneous endoscopic gastroenterostomy
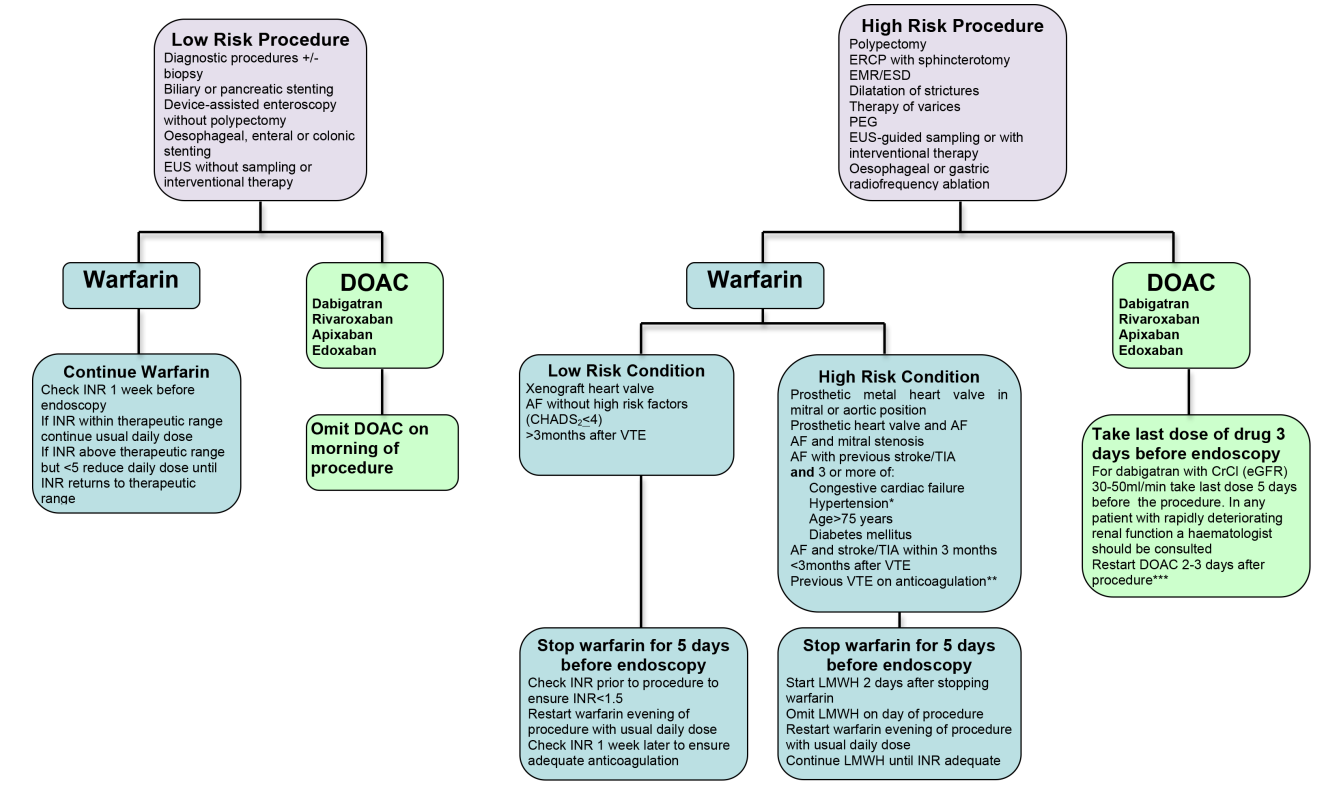
Figure 2: Guidelines for the management of patients on warfarin or Direct Oral Anticoagulants (DOAC) undergoing endoscopic procedures: 2021 update [7]
*Blood pressure >140/90mmHg or on antihypertensive medication
**Previous VTE on anticoagulation and target INR now 3.5
***depends on haemorrhagic and thrombotic risk, interval may be extended for ESD
EUS = endoscopic ultrasound, ERCP = endoscopic retrograde cholangiopancreatography, EMR = endoscopic mucosal resection, ESD = endoscopic submucosal dissection, PEG = percutaneous endoscopic gastroenterostomy, INR = international normalised ratio, AF = atrial fibrillation, VTE = venous thromboembolism, TIA = transient ischaemic attack, LMWH = low molecular weight heparin.
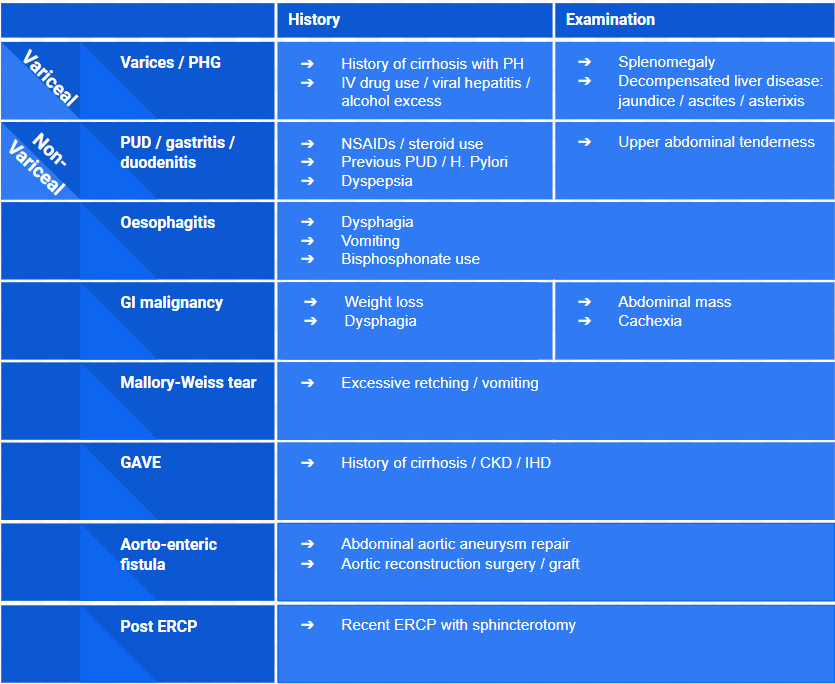
Figure 3: Causes of AUGIB with important history and examination features
CKD = chronic kidney disease, IHD = ischaemic heart disease, NSAIDs = non-steroidal anti-inflammatory drugs, PH = portal hypertension, PHG = portal hypertensive gastropathy, PUD = peptic ulcer disease.
Non-variceal upper gastrointestinal bleeding
Non-variceal upper gastrointestinal bleeding (NVUGIB) comprises the majority of AUGIB cases. The most common cause is due to gastric and duodenal erosions / ulceration as a result of non steroidal anti-inflammatory drugs (NSAIDS) or infection with Helicobacter pylori (H. pylori).[8] Removal of causative medications and the eradication of H.pylori may prevent future peptic ulcer disease and bleeding. [9]
- Proton pump inhibitors (PPI) (Figure 4)
Acidic environments are thought to adversely affect platelet aggregation and blood coagulation. PPI work by increasing intragastric pH, which promotes platelet aggregation and improves conditions for ulcer healing. [10]
The National Institute for Clinical Excellence (NICE) and BSG guidelines do not recommend the use of PPI pre-endoscopy in those presenting with AUGIB.[2,6] This recommendation is based on a 2010 Cochrane review of six trials, concluding that PPI infusion pre-endoscopy showed a reduction of stigmata of recent haemorrhage and the need for intervention at endoscopy. [11] Therefore, there is concern that PPIs pre-endoscopy may obscure potential targets for endoscopic therapy. The review also concluded that pre-endoscopic PPIs in NVUGIB did not improve rates of re-bleeding, surgery, or mortality when compared with standard care.[11] The European Society of Gastrointestinal Endoscopy (ESGE) recently reviewed their stance on pre-endoscopic PPI therapy, recommending that high-dose intravenous PPI be considered pre-endoscopy in acute upper GI haemorrhage. This change was prompted by a lack of high-level evidence supporting the impact of pre-endoscopic PPI on clinically relevant patient outcomes, and aligns with other NVUGIB guideline recommendations. [12]
Confirmed peptic ulcer disease should be treated with a regime of high dose PPI. A meta-analysis conducted by Tringali et al concluded that when comparing intravenous (IV) and oral administration of PPI, there were no differences in re-bleed rates, 30-day mortality, need for repeat endoscopy or surgical intervention.[13] Bleeding peptic ulcers are usually treated on high doses for 4-8 weeks, and long term gastroprotection should be considered. The method of PPI administration should therefore be individualised for the patient, taking into consideration co-morbidities which may affect compliance (confusion, dysphagia) and findings of high-risk stigmata on endoscopy.

Figure 4: PPI equivalents to 20mg omeprazole, and lowest available doses.[14]
- Helicobacter Pylori eradication
H. Pylori are commonly implicated in peptic ulcer disease (up to 90% of duodenal and 70% of gastric ulcers[15,16]) and eradication has been shown to reduce ulcer recurrence and rebleeding[17,18]. Before initiating treatment, suspicion of H. Pylori infection should be confirmed by a campylobacter-like organism (CLO) test or gastric biopsy at endoscopy. Alternatively, a stool antigen test (SAT) can be used. When H. Pylori infection is detected, eradication therapy should begin immediately and consists of high dose oral PPI and a combination of antibiotics. Amoxicillin and clarithromycin are commonly used, however, due to variations in antimicrobial resistance, local, trust specific guidelines should be consulted. [8]
- Histamine Type 2 Receptor Antagonists e.g. ranitidine
H2 antagonists are used as an alternative to PPIs for gastro-oesophageal reflux disease (GORD) and in the primary and secondary prevention of peptic ulcers. A meta-analysis conducted by Zhang et al concluded that re-bleeding (OR = 0.36; 95%CI: .25-0.51) and need for surgical intervention (OR = 0.29; 95%CI: 0.09-0.96) was lower in PPIs compared with H2 antagonists after successful endoscopic treatment of gastric ulcers. However, there was no difference in overall mortality. [19] Similar findings were seen by Gisbert et al, but only in higher grade ulcers and when adjuvant sclerotherapy was not used at endoscopy. It was concluded that the data was not powerful enough to recommend a superior class of drug. [20] Therefore, H2 antagonists should be considered where there is a contraindication to PPI therapy (ie. allergy or intolerance).
- Sucralfate
Sucralfate is a complex of aluminium hydroxide and sulfated sucrose which forms a physical barrier to protect damaged mucosa from acid, pepsin and bile acid injury. Sucralfate may provide adjunctive benefit in patients with persistent UGI inflammation despite PPI therapy, or where acid suppression therapy is contraindicated.[21]
- Potassium competitive acid blockers (PCAB) e.g. vonoprazan
Potassium competitive acid blocker (PCAB) agents are a novel class of acid-suppression treatment which has been shown to be at least as effective as PPI therapy for H. pylori eradication and erosive oesophagitis.[22,23] They have a potent acid suppression effect and therefore offer promise for the future, either in combination with PPIs or as an alternative.
- Tranexamic acid
Tranexamic acid is an anti-fibrinolytic agent which is indicated for use in trauma and postpartum haemorrhage. The HALT-IT trial showed no mortality benefit with tranexamic acid when used in AUGIB but found a higher risk of venous thromboembolic versus placebo (0.8% vs. 0.4%).[24]. Tranexamic acid is therefore not recommended for use in AUGIB.
Acute variceal upper gastrointestinal bleeding
- Terlipressin
Terlipressin is a vasopressin agonist which can be given intravenously as boluses or as a continuous infusion to reduce portal pressures in variceal bleeding. Terlipressin has a better side effect profile compared to vasopressin and has a lower risk of systemic toxicity.[25] Terlipressin causes vasoconstriction in splanchnic arterioles by binding to v1 receptors in the smooth muscle. Subsequently, splanchnic blood flow and portal pressures are reduced, causing an increase in systemic vascular resistance but not affecting cardiac output.[26,27] For this reason it should be used cautiously in patients with heart failure, coronary artery disease or peripheral vascular disease. A Cochrane meta-analysis conducted by Ioannou et al concluded that terlipressin was associated with a reduction in all cause mortality when compared with placebo (relative risk 0.66, 95% CI 0.49 to 0.88).[28] BSG and NICE recommend that terlipressin should be started when variceal bleeding is suspected (at least 30 minutes before endoscopy) and to continue for 2-5 days if variceal bleeding is confirmed endoscopically. The recommended dose is 2mg four times a day (QDS) for 48 hours, then reducing to 1mg QDS for 3 days.[2]
- Somatostatin and Octreotide
Somatostatin and its analogue (Octreotide) are rarely used in the UK for AUGIB, but are recommended as first line agents in AVUGIB by the American College of Gastroenterology (ACG) and American Association Study for Liver Disease (AASLD). [29] The mechanism is thought to be similar to that of terlipressin: portal blood flow and portal pressure is reduced through splanchnic vasoconstriction. Somatostatin has a short half life so must be given as a continuous IV infusion. Octreotide can be given as IV or subcutaneous injections, but a continuous infusion is recommended in AVUGIB. Patients receiving octreotide require cardiac monitoring due to the potential for atrioventricular node blockade, and blood glucose monitoring due to the inhibitory action on glucagon and insulin.[30] A large multicentre trial conducted by Seo et al concluded that the haemostatic efficacy of terlipressin, somatostatin and octreotide are equivalent in AVUGIB, but with a higher incidence of hyponatremia in those receiving terlipressin.[31]
- Antibiotics
Bacterial infections are common in patients with cirrhosis presenting with AVUGIB: 20% of patients at 48 hours and nearly 36% at 7 days.[32] Moreover, concurrent infection with AVUGIB carries a significantly increased mortality (47.8% vs 14.6%) and re-bleed risk (43.5% vs 9.8%).[32] NICE and BSG therefore recommend the use of empirical antibiotics at presentation of those patients presenting with suspected AVUGIB. Fluoroquinolones (such as ciprofloxacin 1g daily) are often used but local antimicrobial policies should be consulted. [33]
Other pharmacological management in AUGIB
- Prokinetics e.g. erythromycin / metoclopramide
Prokinetics may improve mucosal visualisation at endoscopy. A meta-analysis of eight studies found that administration of erythromycin reduced the need for ‘second-look’ endoscopy (15.1% vs 25%, OR 0.51; 95% CI:0.34-0.77) and increased the rates of ‘adequate mucosal visualisation’ (OR 4.1, 95% CI 2.0-8.5).[34,35] Erythromycin 250mg IV 30-120 minutes pre-endoscopy is recommended by the European Society of Gastroenterology (ESGE), but not by NICE or BSG. Erythromycin should be used with caution in those with prolonged QT interval, macrolide sensitivity and concomitant use of digoxin or statins. Prokinetics may be particularly helpful in patients who require emergency endoscopy but with insufficient fasting time, however, this should be used alongside tracheal intubation to protect the airway from gastric aspiration. There is insufficient evidence on the use of metoclopramide in AUGIB.
- Iron replacement
Iron replacement accelerates recovery of anaemia and should be considered for patients with AUGIB and anaemia following endoscopic therapy.[36–38] Normalisation of haemoglobin levels is faster with intravenous iron versus oral iron,[37] and should be considered especially in patients with more pronounced anaemia (e.g. Hb <100g/L).
- Cessation of drugs
In AUGIB, the BSG recommends that low dose aspirin be continued. A 3-fold increase in cardiovascular or cerebrovascular events was seen when aspirin secondary prophylaxis was held; the majority of events at 7-10 days. [2] Conversely, the ESGE recommends aspirin be temporarily held in cases of suspected AVUGIB. The decision to restart aspirin when suspended, should be taken after consideration of individual patient risk factors. [39]
P2Y12 inhibitors (i.e. Clopidogrel, ticagrelor) should be temporarily held in all acute GI bleeding, except in patients with coronary artery stents, where the risks and benefits should be discussed with cardiology. Where P2Y12 inhibitors have been suspended, the BSG and ESGE recommend restarting within 5 days owing to the risk of stent occlusion [2,39]
Anticoagulants (I.e. warfarin and direct acting oral anticoagulants) should be suspended in cases of suspected acute upper GI bleeding. [2,39] Again, individual patient risk factors should be considered when deciding when to restart anticoagulants. Importantly, whatever decision is reached must be clearly documented and communicated to the patient and other involved healthcare professionals. [2]
Conclusion
Evidence-based pharmacological treatment measures exist in AUGIB which can improve patient outcome by reducing rebleeding risk and mortality (Figure 5). These may be delivered by frontline clinicians prior to endoscopy following variceal vs non-variceal risk stratification as per the BSG AUGIB care bundle, and following an endoscopic diagnosis. Clinicians should be aware of these measures and be proactive at reviewing the endoscopy reports to guide medical management.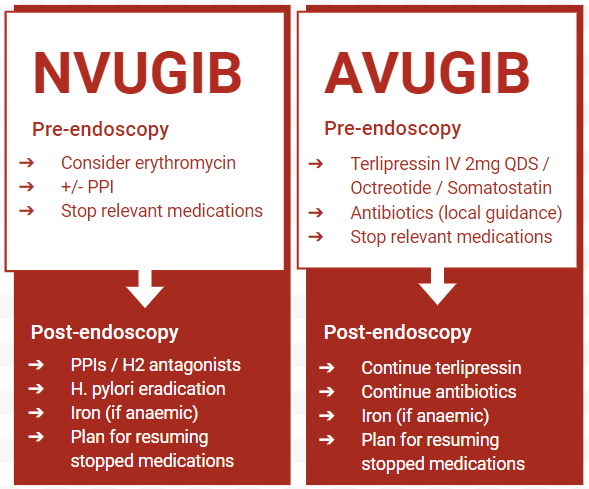
Figure 5: Summary of pharmacological management of AUGIB. AVUGIB = acute variceal upper gastrointestinal bleed, NVUGIB = non variceal upper gastrointestinal bleed, PPI = proton pump inhibitor.
Author Biographies
Dr Jacob Flapan

Dr Ria Smith
Ria is a gastroenterology trainee registrar working at University Hospital Plymouth, currently completing the advanced hepatology training post.

Dr Keith Siau
Consultant Gastroenterologist at Royal Cornwall Hospitals NHS Trust and BSG Endoscopy committee member with interests in endoscopy training. Serves on the editorial board of Endoscopy, Endoscopy International Open, UEG Journal and Frontline Gastroenterology. Often seen on Twitter @drkeithsiau.
CME
IBD Surveillance Colonoscopy – This is how I do it
03 December 2024
Masterclass - Colonic stents - who, when and where
02 September 2024
- Hearnshaw SA, Logan RFA, Lowe D, et al. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut. 2011;60:1327–35.
- Siau K, Hearnshaw S, Stanley AJ, et al. British Society of Gastroenterology (BSG)-led multisociety consensus care bundle for the early clinical management of acute upper gastrointestinal bleeding. Frontline Gastroenterol. 2020;11:311–23.
- Baradarian R, Ramdhaney S, Chapalamadugu R, et al. Early intensive resuscitation of patients with upper gastrointestinal bleeding decreases mortality. Am J Gastroenterol. 2004;99:619–22.
- Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for uppergastrointestinal haemorrhage. Lancet. 2000;356:1318–21.
- Vreeburg EM, Terwee CB, Snel P, et al. Validation of the Rockall risk scoring system in upper gastrointestinal bleeding. Gut. 1999;44:331–5.
- Dworzynski K, Pollit V, Kelsey A, et al. Management of acute upper gastrointestinal bleeding: summary of NICE guidance. BMJ. 2012;344:e3412.
- Veitch AM, Radaelli F, Alikhan R et al. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guideline update. Gut. 2021;70(9):1611-1628.
- Gralnek IM, Dumonceau J-M, Kuipers EJ, et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47:a1–46.
- Lee Y-C, Dore MP, Graham DY. Diagnosis and Treatment of Helicobacter pylori Infection. Annu Rev Med. 2022;73:183–95.
- Green FW Jr, Kaplan MM, Curtis LE, et al. Effect of acid and pepsin on blood coagulation and platelet aggregation. A possible contributor prolonged gastroduodenal mucosal hemorrhage. Gastroenterology. 1978;74:38–43.
- Sreedharan A, Martin J, Leontiadis GI, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2010;2010:CD005415.
- Gralnek IM, Stanley AJ, Morris AJ, et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2021. Endoscopy. 2021;53:a1369-5274.
- Tringali A, Manta R, Sica M, et al. Comparing intravenous and oral proton pump inhibitor therapy for bleeding peptic ulcers following endoscopic management: a systematic review and meta-analysis. Br J Clin Pharmacol. 2017;83:1619–35.
- Graham DY, Tansel A. Interchangeable Use of Proton Pump Inhibitors Based on Relative Potency. Clin Gastroenterol Hepatol. 2018;16:800–8.e7.
- Graham DY, Klein PD, Opekun AR, et al. Effect of age on the frequency of active Campylobacter pylori infection diagnosed by the [13C]urea breath test in normal subjects and patients with peptic ulcer disease. J Infect Dis. 1988;157:777–80.
- Marshall BJ, McGechie DB, Rogers PA, et al. Pyloric Campylobacter infection and gastroduodenal disease. Med J Aust. 1985;142:439–44.
- Gisbert JP, Khorrami S, Carballo F, et al. Meta-analysis: Helicobacter pylori eradication therapy vs. antisecretory non-eradication therapy for the prevention of recurrent bleeding from peptic ulcer. Aliment Pharmacol Ther. 2004;19:617–29.
- Ford AC, Delaney BC, Forman D, et al. Eradication therapy for peptic ulcer disease in Helicobacter pylori positive patients. Cochrane Database Syst Rev. 2006;CD003840.
- Zhang Y-S, Li Q, He B-S, et al. Proton pump inhibitors therapy vs H2 receptor antagonists therapy for upper gastrointestinal bleeding after endoscopy: A meta-analysis. World J Gastroenterol. 2015;21:6341–51.
- Gisbert JP, González L, Calvet X, et al. Proton pump inhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleeding peptic ulcer. Aliment Pharmacol Ther. 2001;15:917–26.
- Blum AL, Bethge H, Bode JC, et al. Sucralfate in the treatment and prevention of gastric ulcer: multicentre double blind placebo controlled study. Gut. 1990;31:825–30.
- Murakami K, Sakurai Y, Shiino M, et al. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: a phase III, randomised, double-blind study. Gut. 2016;65:1439–46.
- Laine L, DeVault K, Katz P, et al. Vonoprazan Versus Lansoprazole for Healing and Maintenance of Healing of Erosive Esophagitis: A Randomized Trial. Gastroenterology. 2023;164:61–71.
- HALT-IT Trial Collaborators. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet. 2020;395:1927–36.
- Zhou X, Tripathi D, Song T, et al. Terlipressin for the treatment of acute variceal bleeding: A systematic review and meta-analysis of randomized controlled trials. Medicine . 2018;97:e13437.
- Møller S, Hansen EF, Becker U, et al. Central and systemic haemodynamic effects of terlipressin in portal hypertensive patients. Liver. 2000;20:51–9.
- Sarin SK, Sharma P. Terlipressin: an asset for hepatologists! Hepatology. 2011;54:724–8.
- Ioannou G, Doust J, Rockey DC. Terlipressin for acute esophageal variceal hemorrhage. Cochrane Database Syst Rev. 2003;CD002147.
- Garcia-Tsao G, Sanyal AJ, Grace ND, et al. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46:922–38.
- Octreotide 100 micrograms/1ml Solution for Injection - Summary of Product Characteristics (SmPC) - (emc). https://www.medicines.org.uk/emc/product/373/smpc (accessed 12 May 2023)
- Seo YS, Park SY, Kim MY, et al. Lack of difference among terlipressin, somatostatin, and octreotide in the control of acute gastroesophageal variceal hemorrhage. Hepatology. 2014;60:954–63.
- Bernard B, Cadranel JF, Valla D, et al. Prognostic significance of bacterial infection in bleeding cirrhotic patients: a prospective study. Gastroenterology. 1995;108:1828–34.
- Jalan R, Hayes PC. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. British Society of Gastroenterology. Gut. 2000;46 Suppl 3-4:III1–15.
- Rahman R, Nguyen DL, Sohail U, et al. Pre-endoscopic erythromycin administration in upper gastrointestinal bleeding: an updated meta-analysis and systematic review. Ann Gastroenterol Hepatol . 2016;29:312–7.
- Bai Y, Guo J-F, Li Z-S. Meta-analysis: erythromycin before endoscopy for acute upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2011;34:166–71.
- Mak LY, Lau CW, Hui YT, et al. Joint recommendations on management of anaemia in patients with gastrointestinal bleeding in Hong Kong. Hong Kong Med J. 2018;24:416–22.
- Bager P, Dahlerup JF. Randomised clinical trial: oral vs. intravenous iron after upper gastrointestinal haemorrhage--a placebo-controlled study. Aliment Pharmacol Ther. 2014;39:176–87.
- Chang A, Rugivarodom M, Pungpipattrakul N, et al. Role of oral iron supplementation for anemia secondary to acute nonvariceal upper gastrointestinal bleeding: a randomized controlled trial. J Gastroenterol Hepatol. 2023;38:1283–91.
- Gralnek IM, Duboc MC, Garcia-Pagan JC, et al. Endoscopic diagnosis and management of esophagogastric variceal haemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2022;54:1094-1120.